
TRAUMA TREATMENT FOUNDATIONAL PHASE-WORK (TTFP)
- Dr. Marie Dezelic and Dr Gabriel Ghanoum
- May 15, 2014
- 8 min read
INTEGRATIVE TRAUMA-INFORMED TREATMENT:
CORE ELEMENTS FOR STABILIZATION, RECOVERY, & RECONNECTION
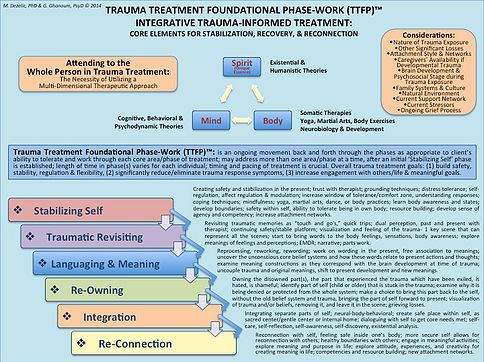
A “Conceptual Pictograph” handout is included as a one-page reference for clinicians, to have as a guide and overview for treatment. This is only a snapshot of the breadth of clinical work that will occur in trauma-informed treatment. A comprehensive list of references is included for education and resources for treatment.
Trauma Treatment Foundational Phase-Work (TTFP) is a model and framework of integrative trauma-informed treatment and therapeutic care combining the most recent, researched information available in the field of trauma treatment and development. It builds upon existing theories and strategies; however, this model utilizes a holistic and existential methodology, attending to the “Whole Person in Trauma Treatment,” which necessitates a multi-dimensional therapeutic approach. Any clinician working in the trauma field understands that they must have a therapeutic toolbox full of treatment interventions, strategies, and skills, as trauma manifests itself in a variety of ways. Often times, the manifestations occur as several diagnosable clinical disorders (not only as PTSD), up to and possibly including a disorganization in personality development and social/relational interactions (personality disorders). Multiple disorders and symptoms are the indications caused by trauma, occurring from developmental trauma, a one-time traumatic event, or chronic traumatic events in adolescence and adulthood. The chronic effects of trauma are often perpetuated by the ongoing symptoms and reactions. One of the most important considerations clinicians must keep in mind is that the variety of maladaptive behaviors that trauma patients engage in, are truly coping strategies for self-regulatory behaviors of sensory and affect management, self-soothing, and desired connection to the outside world. If these behaviors are removed too quickly in treatment, and are not replaced with behaviors that trauma patients can tolerate, accept, and work with for self-regulation, they will manifest in other ways or increase in propensity.
Trauma Treatment Foundational Phase-Work (TTFP) : developed by the authors, is defined as an ongoing “movement” back and forth through the phases as appropriate to client’s ability to tolerate and work through each core area/phase of treatment; clinicians may address more than one area/phase at a time, after an initial ‘Stabilizing Self’ phase is established for the patient; length of time in phase(s) varies for each individual; timing and pacing of treatment is crucial, as each individual is unique and needs to be guided and assisted rather than pushed to overcome new areas. The overall trauma-informed treatment goals are: (1) build safety, stability, self-regulation & flexibility, (2) significantly reduce/eliminate trauma response symptoms, (3) increase engagement with others/life and meaningful goals.
Whole Person in Trauma Treatment:
Treatment addresses the Whole person: Mind, Body, and Spirit (Unique Essence—Existence). Trauma-informed treatment is not a specific theory; it is a treatment style based on a range of theoretical and psychological models, incorporating several techniques, addressing a variety of symptoms and issues. In doing so, there are several therapeutic theories that are utilized and combined throughout treatment, these include: (1) Mind: Cognitive, Behavioral, and Psychodynamic theories; (2) Body: Somatic therapies, Yoga, Martial Arts, Body Exercises, Neurobiology & Development; (3) Spirit (Unique Existential Essence): Existential and Humanistic theories. Attending to the whole person in trauma-informed treatment offers the possibility of true and lasting recovery, healing and engagement.
Considerations:
There are several considerations that will impact how the patient is able to tolerate each area/phase of treatment. Clinical judgment should be used in incorporating or adjusting to each of the considerations during the trauma treatment. These considerations include: Nature of Trauma Exposure; Other Significant Losses; Attachment Style & Networks; Caregivers’ Availability if Developmental Trauma; Brain Development & Psychosocial Stage during Trauma Exposure; Family Systems & Cultural Implications; Natural Environment; Current Support Network; Current Stressors; Ongoing Grief Process.
Trauma Treatment Foundational Phase-Work (TTFP) Model:
The initial ‘Stabilizing Self’ area/phase of treatment must be completed before moving on to the rest of the areas, and will likely be an ongoing phase of treatment and care. Patients must learn to “be” and live in their own bodies, and begin to develop an ability to tolerate and modulate physiological sensations and arousal, before any trauma processing work can be done. Trauma-informed therapy must include an element of ‘Traumatic Revisiting,’ offered in a variety of interventions and techniques. If this area is left out, it is not truly trauma treatment. The additional areas/phases are significant ongoing working areas that will overall increase one’s: self-confidence, self-efficacy, agency, ability to tolerate and understand self and relationships with the world, engagement with others and activities; and likewise assist in decreasing one’s: sense of shame, guilt, brokenness, loathing, anger, hatred, fear, confusion, distrust, chaotic disregulation, and chronic maladaptive, harmful behaviors. Keep in mind that although a later phase is reached, new changes to self, environment, and behaviors, may trigger other trauma material, which may not have surfaced until these areas/phases; this will necessitate ‘Traumatic Revisiting’ and working through the new trauma memories. This is precisely why trauma treatment is an ongoing movement between the areas/phases.
Trauma-informed therapy will include a considerable amount of grief work and processing throughout the areas/phases. As symptoms begin to shift or are removed, there will be a grief process revolving around several elements: the absence of or loss of connections to caregivers and others, loss and changes of self, loss of time, loss of activities and choices in life, due to the trauma exposure and maintenance of symptoms.
Stabilizing Self:
Creating safety and stabilization in the present; trust with therapist; grounding techniques; distress tolerance; self-regulation, affect regulation & modulation; increase window of tolerance/comfort zone, understanding responses; coping techniques; mindfulness; yoga, martial arts, dance, or body practices; learn body awareness and states; develop boundaries; safety within self, ability to tolerate being in own body; resource building; develop sense of agency and competency; increase attachment networks.
Traumatic Revisiting:
Revisiting traumatic memories as “touch and go's,” quick trips; dual perception, past and present with therapist; continuing safety/stable platform; visualization and feeling of the trauma- 1 key scene that can represent all the scenes; start to bring words to the body feelings, sensations, body awareness; explore meanings of feelings and perceptions; EMDR; narrative; parts work.
Languaging & Meaning:
Reprocessing, reworking, rewording; work on wording in the present, free association to meanings; uncover the unconscious core belief systems and how these words relate to present actions and thoughts; examine meaning constructions (biological, personal, social/relational, and cultural) as they correspond with the brain development at time of trauma; uncouple trauma and original meanings, shift to present development and new meanings.
Re-Owning:
Owning the disowned part(s), the part that experienced the trauma which have been exiled, is hated, is shameful; identify part of self (child or older) that is stuck in the trauma; examine why it is being denied or protected from the whole system; make a choice to bring this part back to the self, without the old belief system and trauma, bringing the part of self forward to present; visualization of trauma and/or beliefs, removing it, and leave it in the scene; grieving losses.
Integration:
Integrating separate parts of self; neural-body-behavioral; create safe place within self, as sacred center/gentle center or internal home; dialoguing with self to get core needs met; self-care, self-reflection, self-awareness, self-discovery, existential analysis.
Re-Connection:
Reconnection with self, feeling safe inside one’s body; more secure self allows for reconnection with others; healthy boundaries with others; engage in meaningful activities; explore meaning and purpose in life; explore attitude, experiences, and creativity for creating meaning in life; competencies and resource building; new attachment networks.
The references listed below, books and workbooks, have aided in informing this model, and are likewise invaluable resources that all trauma clinicians should have in their library and as sources of information for informing treatment interventions, strategies and techniques. Each area/phase of treatment can be expounded upon utilizing these mentioned resources. Clinicians should receive training and supervision to understand core concepts in trauma before attempting to offer trauma-informed treatment.
References:
Blaustein, M. E., & Kinniburgh, K. M. (2010). Treating traumatic stress in children and adolescents: How to foster resilience through attachment, self-regulation, and competency. New York: The Guilford Press.
Boon, S., Steele, K., & van der Hart, O. (2011). Coping with trauma-related dissociation: Skills training for patients and their therapists. New York: W. W. Norton & Company, Inc.
Curran, L. A. (2013). 101 trauma-informed interventions: Activities, exercises and assignments to move the client and therapy forward. Eau Claire, WI: PESI, LLC.
Curran, L. A. (2010). Trauma competency: A clinician’s guide. Eau Claire, WI: PESI, LLC.
Dezelic, M. S. (2014). Meaning-centered therapy workbook: Based on Viktor Frankl’s logotherapy and existential analysis. San Rafael, CA: Palace Printing and Design.
Fisher, S. F. (2014). Neurofeedback in the treatment of developmental trauma: Calming the fear-driven brain. New York: W. W. Norton & Company, Inc.
Foa, E. B., Keane, T. M., Friedman, M. J., & Cohen, J. A. (Eds.) (2009). Effective treatments for PTSD: Practical guidelines from the International Society for Traumatic Stress Studies, Second Edition. New York: The Guilford Press.
Frankl, V. E. (2010). The feeling of meaninglessness: A challenge to psychotherapy and philosophy. Alexander Batthyany (Ed.). Milwaukee, WI: Marquette University Press.
Frankl, V. E. (2006). Man’s search for meaning. Boston, Massachusetts: Beacon Press.
Frankl, V. E. (2004). On the theory and therapy of mental disorders: An introduction to logotherapy and existential analysis (James M. Dubois, Translation). New York: Brunner-Routledge.
Frankl, V. E. (2000). Man’s search for ultimate meaning. New York: Perseus Publishing.
Frankl, V. E. (1988). The will to meaning: Foundations and applications of logotherapy (Expanded Ed.). New York: Penguin Books USA Inc.
Graber, A. V. (2004). Viktor Frankl’s logotherapy: Method of choice in ecumenical pastoral psychotherapy (2nd Ed.). Lima, Ohio: Wyndham Hall Press.
Heller, L., & LaPierre, A. (2012). Healing developmental trauma: How early trauma affects self-regulation, self-image, and the capacity for relationship. Berkeley, CA: North Atlantic Books.
Herman, J. (1997). Trauma and recovery: The aftermath of violence—from domestic abuse to political terror. New York: Basic Books.
Levine, P. A. (2010). In an unspoken voice: How the body releases trauma and restores goodness. Berkeley, CA: North Atlantic Books.
Levine, P. A. (2005). Healing trauma: A pioneering program for restoring the wisdom of your body. Boulder, CO: Sounds True.
Levine, P. A. (1997). Waking the tiger: Healing trauma. Berkeley, CA: North Atlantic Books.
Lukas, E. (2000). Logotherapy textbook: Meaning-centered psychotherapy consistent with the principles outlined by Viktor E. Frankl, MD, Concept of human beings and methods in logotherapy (Theodor Brugger, Translation). Toronto, Canada: Liberty Press.
Mendelsohn, M., Herman, J. L., Schatzow, E., Coco, M., Kallivayalil, D., & Levitan, J. (2011). The trauma recovery group: A guide for practitioners. New York: The Guilford Press.
Ogden, P., Minton, K., & Pain, C. (2006). Trauma and the body: A sensorimotor approach to psychotherapy. New York: W. W. Norton & Company, Inc.
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. New York: W. W. Norton & Company, Inc.
Raja, S. (2012). Overcoming trauma and PTSD: A workbook integrating skills from ACT, DBT, and CBT. Oakland, CA: New Harbinger Publications, Inc.
Rothschild, B. (2000). The body remembers: The psychophysiology of trauma and trauma treatment. New York: W. W. Norton & Company, Inc.
Scaer, R. (2005). The trauma spectrum: Hidden wounds and human resiliency. New York: W. W. Norton & Company, Inc.
Schwartz, R. C. (1995). Internal family systems therapy. New York: The Guilford Press.
Shapiro, F. (2001). Eye movement desensitization and reprocessing: Basic principles, protocols, and procedures. New York: The Guilford Press.
Shapiro, R. (2010). The trauma treatment handbook: Protocols across the spectrum. New York: W. W. Norton & Company, Inc.
Shore, A. (1994). Affect development and the origin of the self: The neurobiology of emotional development. Hillsdale, NJ: Lawrence Erlbaum.
Siegel, D. J. (2012). Pocket guide to interpersonal neurobiology: An integrative handbook of the mind. New York: W. W. Norton & Company, Inc.
Siegel, D. J. (2011). Mindsight: The new science of personal transformation. New York: Bantam Books Trade Paperbacks.
Solomon, M. F., & Siegel, D. J. (Eds.) (2003). Healing trauma: Attachment, mind, body, and brain. New York: W. W. Norton & Company, Inc.
van der Kolk, B. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. New York: Viking.
Van der Kolk, B., McFarlane, A. C., & Weisaeth, L. (Eds.) (2006). Traumatic stress: The effects of overwhelming experience on mind, body, and society. New York: The Guilford Press.
Williams, M. B., & Poijula, S. (2002). The PTSD workbook: Simple, effective techniques for overcoming traumatic stress symptoms. Oakland, CA: New Harbinger Publications, Inc.
These Handouts are meant for Mind-Body-Spirit (bio-psycho-social-spiritual) awareness and self-help empowerment. ENJOY!
No part of the material provided constitutes or replaces psychological and medical services. In the event that you experience distress or unpleasant symptoms, seek professional help immediately.
Reproduction of any material herein must contain the designated U.S. copyright information by the author(s).
If you wish to publish it or use it for your website, please contact the author(s) for permission at:info@drmariedezelic.com
All rights reserved. Tous droits réservés.
No part of these publications may be reproduced through any mechanical, photographic, electronic or phonographic process, stored in a retrieval system or transmitted in any form, without prior written permission from the copyright owner, except in the case of brief quotations embodied in articles or reviews. Unauthorized usage is prohibited. For permission or additional information contact info@drmariedezelic.com.



Comments